Many women with early breast cancer have a very low risk of a locoregional recurrence five years after surgery
23 Mar 2018
Barcelona, Spain: Women with small, low grade, well-defined breast tumours and a genetic profile that shows they are at low risk of the cancer metastasising have only a 1.4% risk of the cancer returning to the site of the original tumour or the nearby lymph nodes (known as locoregional recurrence) within five years, according to new results from a large randomised trial of nearly 7000 patients.
This low risk of locoregional recurrence was seen regardless of whether the women had a mastectomy (the whole breast removed) or breast conserving surgery, in which just the tumour and some surrounding tissue are removed, followed by radiotherapy of the whole breast.
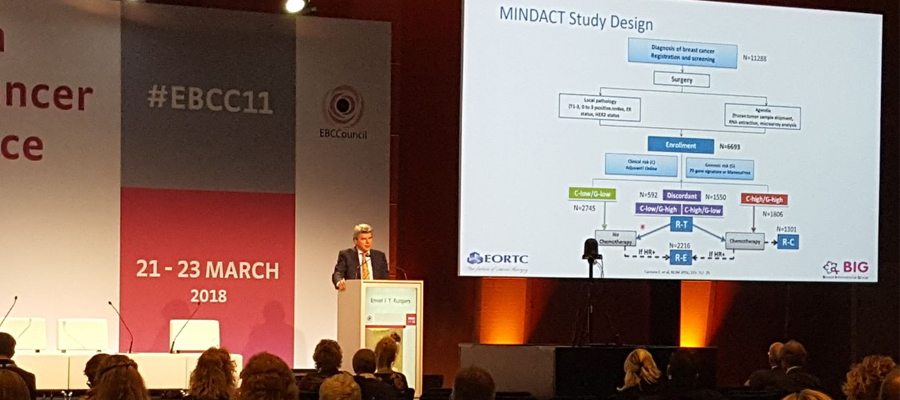
Presenting the latest results from the MINDACT trial [1] at the 11th European Breast Cancer Conference, Professor Emiel Rutgers, a surgeon at the Netherlands Cancer Institute in Amsterdam (The Netherlands), said the findings meant that it was possible to identify women who could safely avoid not only chemotherapy after surgery, but possibly also radiotherapy – both toxic treatments that can have debilitating effects on women’s physical and mental well- being and quality of life.
“These findings show that, for these selected women, breast conservation is as good as mastectomy, and the risk of relapse is so low that we should look for ways of giving them less aggressive treatment. For instance, even though radiotherapy reduces the risk of locoregional recurrence two- to three-fold, can we do without it in some selected patients, such as these low risk women, and also in some women aged over 50 with small tumours, less than 2cms in diameter, who have a 1.4% risk of relapse within five years as well,” said Prof Rutgers.
Among 6693 patients enrolled in the MINDACT trial, 5470 (82%) underwent breast conserving surgery and 1223 (18%) mastectomy. Decisions on how the women were treated were made on the basis of the tumour characteristics (size, grade, hormonal and HER2 status, and whether or not the disease had spread to any lymph nodes). In addition, their genetic make-up was investigated using the 70-gene-signature test (MammaPrint®). This analyses the activity of certain genes in early breast cancer and has been shown to accurately predict the risk of the cancer spreading (metastasising) to other parts of the body within five or ten years.
Women who were at low risk of a recurrence, based on these clinical and genomic factors, did not receive chemotherapy after surgery, while those who were at high risk, did. Women with a mixture of high and low risk factors were randomised to receive chemotherapy or not. Almost all women who had breast conserving surgery also had radiotherapy, but not all of the women who had a mastectomy.
In this latest part of the study, Prof Rutgers and his colleagues looked at the rate of locoregional recurrences five years after surgery and analysed them according to the clinical and genetic characteristics. They found that women who had breast conserving surgery had an overall 2.1% risk of recurrence by five years, but if they had a low 70-gene signature score, the risk dropped to 1.4%, while if they had a high score the risk was 3.6%. Among women who had a mastectomy, the overall risk of recurrence was 2.5%, but this dropped to 0.7% in those with a low genetic score and went up to 4.9% in those with a high score. After full statistical analysis, tumour grade and size were the only factors significantly associated with the risk of locoregional recurrences.
Prof Rutgers said: “The importance of this MINDACT analysis is that local and regional control, in which breast cancer does not come back in the preserved breast, or in the skin after mastectomy, or in the surrounding lymph nodes, is extremely good. The odds of the cancer coming back are about 2% in five years after breast conservation and 2.5% after mastectomy. This includes relapses in the surrounding lymph nodes. This very low risk is determined by the biology of the primary cancer, such as grade, size and growth pattern, and to some extent also by age, with women over 50 years also having a lower overall risk. Among these women aged over 50, those with slow-growing ‘lazy’ breast cancers have a 0.88% risk, and those with more aggressive ones have a 3.5% risk at five years. We should remember that some 10-15 years ago a 10% recurrence rate at 10 years was considered the norm.
“Another important message from these findings is that well-performed breast conserving surgery in women with good indications is as good as mastectomy. Doing a mastectomy when you could very well perform breast conservation will not add a day to the life of a breast cancer survivor.
“This is a wonderful trial that provides wonderful opportunities for further research.”
As a result of these findings, Prof Rutgers says that a study should be performed that prospectively investigates whether women at low risk of a recurrence could avoid radiotherapy.
“For instance, could a woman with an early grade, small tumour, perhaps with a low risk 70- gene signature score, only have breast conserving surgery, and no radiotherapy or chemotherapy? I believe she could. I would very much support a study of women between the ages of 50-70 years with ‘lazy’ small, low grade tumours, in whom the cancer has been completely excised with cancer-free margins. They would receive only hormone therapy and no radiotherapy if the 70-gene signature score shows them as having a low risk. With 1000 patients, such a trial could come to a practice-changing conclusion,” he said.
Chair of the conference, Professor Robert Mansel, Emeritus Professor of Surgery in Cardiff University School of Medicine, Cardiff. UK, who was not involved with the study, commented: “These latest results from the MINDACT trial show the benefits to patients of large, international trials that have the power to detect whether or not it is possible to treat some women safely with less aggressive therapies. Professor Rutgers and colleagues have shown that there is a group of breast cancer patients who are low risk of locoregional recurrence and might be able to avoid radiotherapy and chemotherapy and the associated adverse side effects. I support his suggestion of a prospective trial to investigate this further in older, low-risk women.”
Abstract no: 2 (Best abstract), “Very low risk of locoregional breast cancer recurrence in the EORTC 10041/BIG 03-04 MINDACT trial: analysis of risk factors including the 70-gene signature”, closing plenary session, Friday, 15.05-16.35 hrs, Picasso room.
[1] “MINDACT” is the “Microarray in Node- Negative and 1 to 3 Positive Lymph Node Disease May Avoid Chemotherapy” (EORTC 10041/ BIG 3-04 MINDACT) study.
The MINDACT trial was supported by grants from the European Commission Sixth Framework Program (FP6-LSHC-CT-2004-503426, to the TRANSBIG Network of Excellence), the Breast Cancer Research Foundation, Novartis, F. Hoffmann–La Roche, Sanofi-Aventis, Eli Lilly, Veridex, the U.S. National Cancer Institute, the European Breast Cancer-Council Breast Cancer Working Group (BCWG grant for the MINDACT biobank), the Jacqueline Seroussi Memorial Foundation for Cancer Research (JSMF;; 2006 JSMF Award), Prix Mois du Cancer du Sein (2004 award), Susan G. Komen for the Cure (SG05-0922- 02), Fondation Belge contre le Cancer (SCIE 2005-27), Dutch Cancer Society (KWF), the Netherlands Genomics Initiative–Cancer Genomics Center (2008-2012), Association le Cancer du Sein, Parlons-en!, the Brussels Breast Cancer Walk-Run and the American Women’s Club of Brussels, NIF Trust, German Cancer Aid, the Grant Simpson Trust and Cancer Research UK, Ligue Nationale contre le Cancer, and the EORTC Cancer Research Fund. Whole-genome analysis was provided by Agendia without cost.
Related News
Professor Benjamin Besse becomes President of EORTC
26 Jun 2026
CCTG, EORTC and UK3CR welcome G7 commitment to accelerate global progress against cancer
24 Jun 2026
EORTC welcomes EU Biotech Act and calls for refinements to enable patient-centred trials
24 Jun 2026
New study confirms a key quality of life tool can be used with adolescents with cancer
9 Jun 2026
“Changing practice, improving lives”: EORTC publishes its Annual Report 2025
8 Jun 2026
This Clinical Trials Day, EORTC announces the upcoming Summit for Clinical Cancer Research
20 May 2026
Long-term EORTC trial challenges assumptions about lymph node radiation therapy in breast cancer
17 May 2026
Multinational study provides new evidence for the value of response-adapted, personalised treatment in Hodgkin lymphoma
1 May 2026
EORTC’s presence at ESTRO 2026
30 Apr 2026
Independent, academic cancer trials are vital to improve patient outcomes worldwide
28 Apr 2026